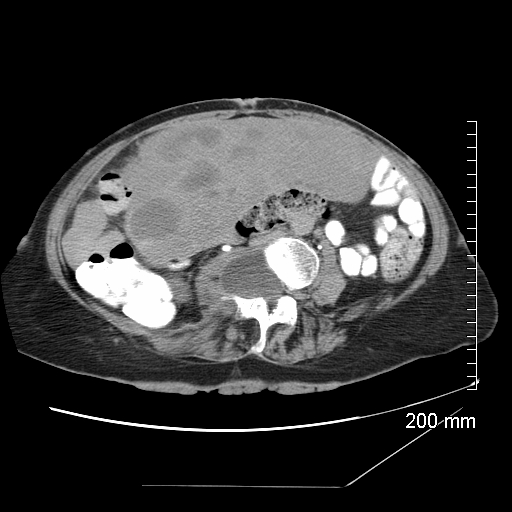
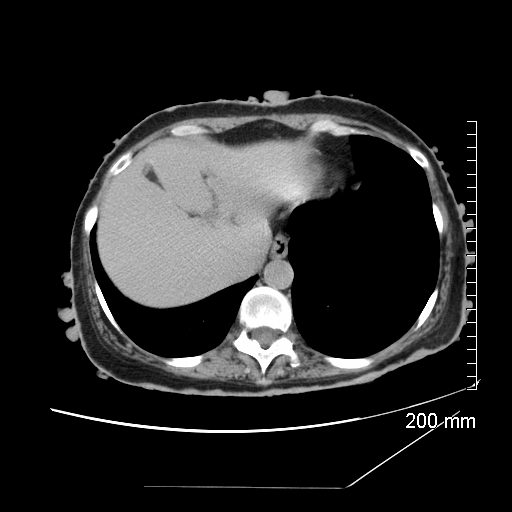
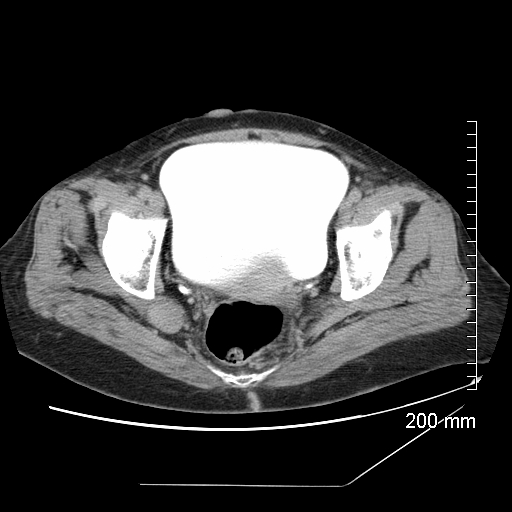
History: 56 year-old post-menopausal female with a complex medical history and an incidentally noted abdominal mass found on a pelvic ultrasound.
Solution: Answers:
1) Neurofibromatosis type-1 (von Recklinghausen disease)
2) Lateral Meningocele, a protrusion of the meninges through a dilated neural foramina, most often occurring with NF-1. A neurenteric cyst is a congenital intraspinal cyst that results from persistent patency of the notochordal canal, and usually exhibit a connection with the spinal canal, with the vertebrae or with the gut by a fibrous stalk.
3) GIST tumor. The most significant risk factor for development of these tumors is the presence of neurofibromatosis type 1. Gastrointestinal involvement in NF1 occurs in three principal forms:
- submucosal/myenteric nerve plexus hyperplasia, mucosal ganglioneuromatosis
- GISTs with varying degrees of neural or smooth-muscle differentiation
- glandular, somatostatin-rich carcinoid in the periampullary region of the duodenum that contains psammoma bodies and may be associated with pheochromocytoma.
In a large series of 156 GISTs, 6.5% of the cases involved coexistent NF1. Typically patients with NF1 have multiple small intestinal GISTs.
R. Sinha, et al. Mesenteric Gastrointestinal Stromal Tumor in a Patient with Neurofibromatosis. AJR 2004; 183:1844-1846
Discussion:
Neurofibromatosis is the most common phakomatosis (neuroectodermal disorder characterized by coexistent skin and CNS tumors). It occurs in 1 in 3000 patients. It affects all 3 germ cell layers and is capable of involving any organ system.
NF-1 (von Recklinghausen disease) results from a defect in Chromosome 17. It accounts for 90% of NF cases, with NF-2 accounting for the other 10%. . Half of these cases result from autosomal dominant inheritence, while the other half occur from spontaneous mutations. In order to meet diagnostic criteria, one must have at least 2 of the following:
- at least 6 café au lait spots
- at least 2 pigmented iris hamartomas (Lisch nodules)
- axillary/inguinal freckling
- at least 2 subcutaneous neurofibromas (or 1 plexiform neurofibroma)
- optic glioma
- first-degree relative with NF-1
- dysplasia of the greater wing of the sphenoid
Classic Triad:
1) Cutaneous lesions
2) Skeletal deformity
3) Mental deficiency
NF-1 radiographic features:
1) CNS
- Optic gliomas (low-grade pilocytic astrocytomas)
- Low-grade brainstem gliomas
- Non-neoplastic hamartomas
2) Spinal cord/canal
- Neurofibromas of exiting nerves
- Dural ectasia
- Low-grade cord astrocytomas
- Lateral meningoceles
3) Skull
- Hypoplastic sphenoid wing
- Macrocrania
4) Plexiform Neurofibromas
- diagnostic of NF1
- most common along CN V peripherally
5) Skeleton
-Erosion of bones/foramina from slow-growing neuromas
-Bowing of tibia/ fibula
-Twisted ribs (ribbon ribs)
6) Chest
-Progressive pulmonary fibrosis
-Intrathoracic meningoceles and neurofibromas
7) Vascular
- Renal artery
stenosis/aneurysm - Abdominal coarctation
8) Abdomen
- Pheochromocytoma
- Carcinoid tumors
- GIST tumors
9) Skin
- Café au lait spots
- Cutaneous neurofibroma
Case and write up courtesy of Dr. Erik Olson
1) Neurofibromatosis type-1 (von Recklinghausen disease)
2) Lateral Meningocele, a protrusion of the meninges through a dilated neural foramina, most often occurring with NF-1. A neurenteric cyst is a congenital intraspinal cyst that results from persistent patency of the notochordal canal, and usually exhibit a connection with the spinal canal, with the vertebrae or with the gut by a fibrous stalk.
3) GIST tumor. The most significant risk factor for development of these tumors is the presence of neurofibromatosis type 1. Gastrointestinal involvement in NF1 occurs in three principal forms:
- submucosal/myenteric nerve plexus hyperplasia, mucosal ganglioneuromatosis
- GISTs with varying degrees of neural or smooth-muscle differentiation
- glandular, somatostatin-rich carcinoid in the periampullary region of the duodenum that contains psammoma bodies and may be associated with pheochromocytoma.
In a large series of 156 GISTs, 6.5% of the cases involved coexistent NF1. Typically patients with NF1 have multiple small intestinal GISTs.
R. Sinha, et al. Mesenteric Gastrointestinal Stromal Tumor in a Patient with Neurofibromatosis. AJR 2004; 183:1844-1846
Discussion:
Neurofibromatosis is the most common phakomatosis (neuroectodermal disorder characterized by coexistent skin and CNS tumors). It occurs in 1 in 3000 patients. It affects all 3 germ cell layers and is capable of involving any organ system.
NF-1 (von Recklinghausen disease) results from a defect in Chromosome 17. It accounts for 90% of NF cases, with NF-2 accounting for the other 10%. . Half of these cases result from autosomal dominant inheritence, while the other half occur from spontaneous mutations. In order to meet diagnostic criteria, one must have at least 2 of the following:
- at least 6 café au lait spots
- at least 2 pigmented iris hamartomas (Lisch nodules)
- axillary/inguinal freckling
- at least 2 subcutaneous neurofibromas (or 1 plexiform neurofibroma)
- optic glioma
- first-degree relative with NF-1
- dysplasia of the greater wing of the sphenoid
Classic Triad:
1) Cutaneous lesions
2) Skeletal deformity
3) Mental deficiency
NF-1 radiographic features:
1) CNS
- Optic gliomas (low-grade pilocytic astrocytomas)
- Low-grade brainstem gliomas
- Non-neoplastic hamartomas
2) Spinal cord/canal
- Neurofibromas of exiting nerves
- Dural ectasia
- Low-grade cord astrocytomas
- Lateral meningoceles
3) Skull
- Hypoplastic sphenoid wing
- Macrocrania
4) Plexiform Neurofibromas
- diagnostic of NF1
- most common along CN V peripherally
5) Skeleton
-Erosion of bones/foramina from slow-growing neuromas
-Bowing of tibia/ fibula
-Twisted ribs (ribbon ribs)
6) Chest
-Progressive pulmonary fibrosis
-Intrathoracic meningoceles and neurofibromas
7) Vascular
- Renal artery
stenosis/aneurysm - Abdominal coarctation
8) Abdomen
- Pheochromocytoma
- Carcinoid tumors
- GIST tumors
9) Skin
- Café au lait spots
- Cutaneous neurofibroma
Case and write up courtesy of Dr. Erik Olson
CT Images