History: 2 month old male with \"reflux\".
Solution: Hypertrophic pyloric stenosis
This is an idiopathic condition and the underlying abnormality is hyperplasia of the circular muscle fibers of the pylorus and gastric antrum. There is about a 5:1 male to female predominance and for whatever reason, it is most frequent in first-born males. Usually manifests as nonbilious projectile vomiting that progresses over time. An experienced clinician will often palpate an olive shaped mass in the region of the pylorus and treatment is surgical.
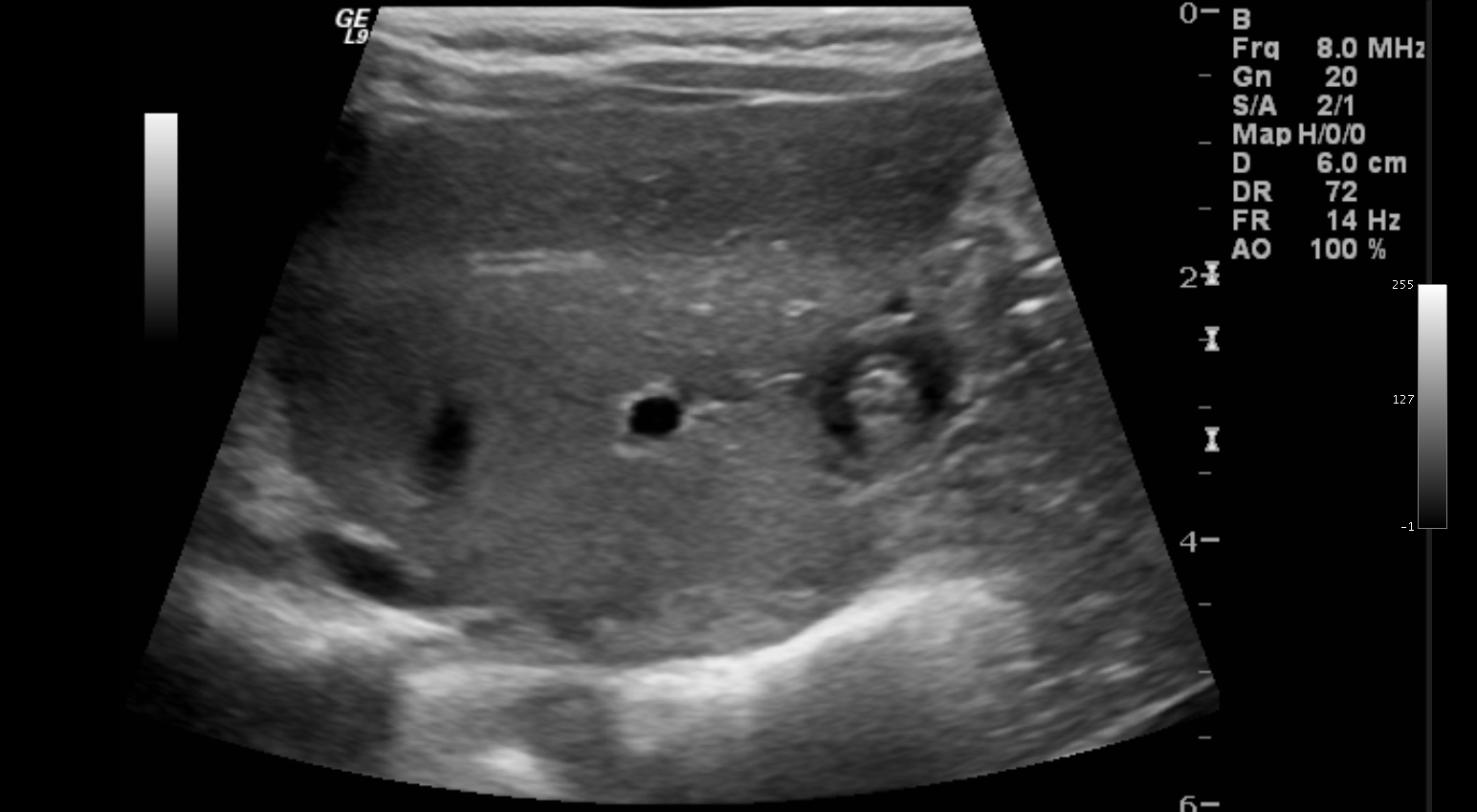
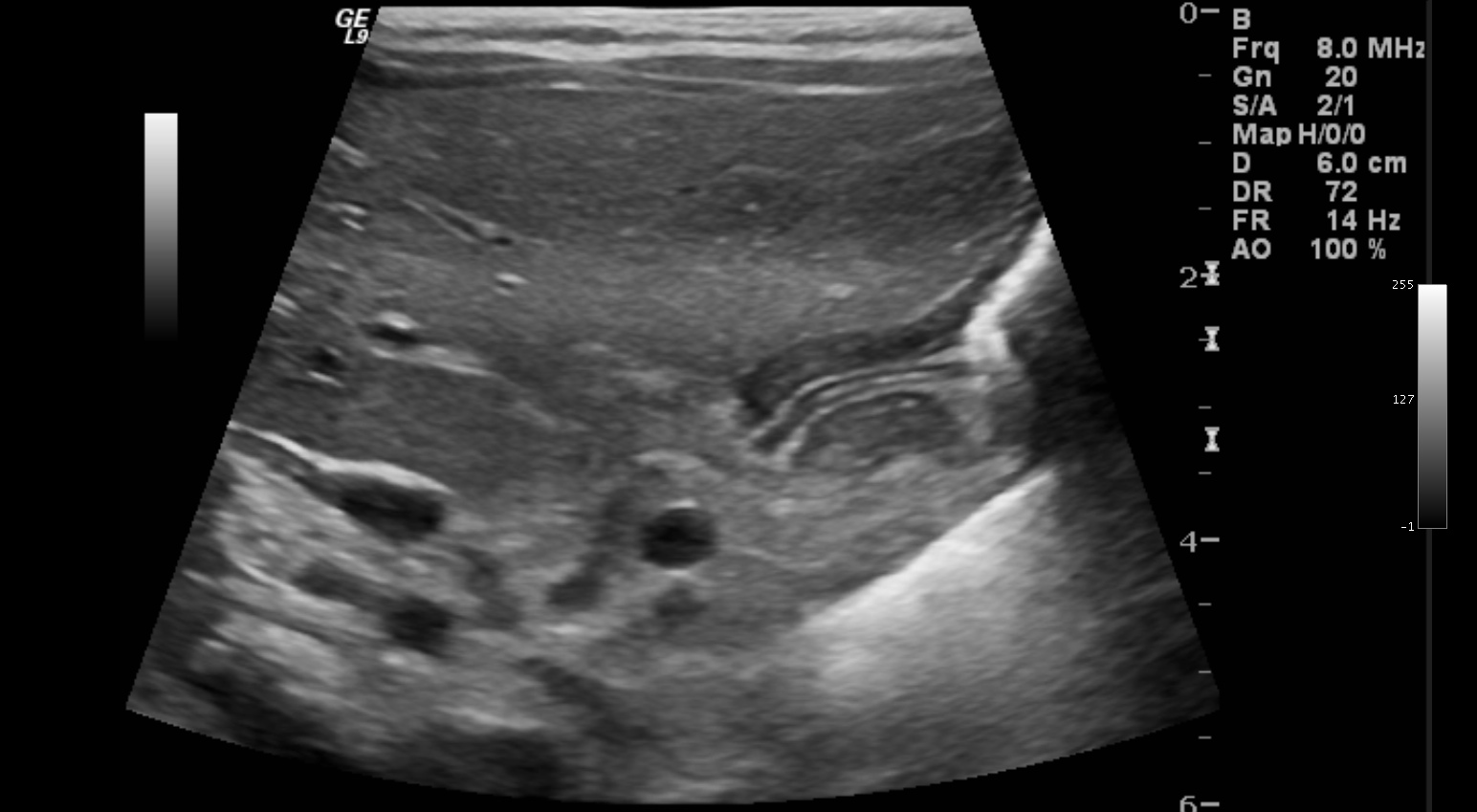
Findings in this case are classic on US with thickened (> 3 mm single wall thickness) pyloric muscular wall and elongated (>15-18 mm depending on how sensitive you want to be) pyloric channel. The first image also shows a \"target sign\" appearance. There have also been calculations based upon pyloric volume, but these are relatively impractical. Most important is to do real-time imaging and identify minimal flow of fluid through the pylorus. Remember to have the patient drinking formula at the time of the examination.
UGI findings include similar findings and there are a plethora of findings described for this condition including: Mushroom sign (appearance of duodenal bulb), teat sign (pointing of the antrum), caterpillar sign (multiple hyper-active muscular contractions in the stomach), shoulder sign (shouldering of the antrum), and diamond sign (focal pointed outpouching in the pyloric channel, which often has a double or triple track appearance). Bottom line is that it is usually obvious if it is there and if you are struggling, it is probably negative. There is actually an adult form as well, although this is less common.
This is an idiopathic condition and the underlying abnormality is hyperplasia of the circular muscle fibers of the pylorus and gastric antrum. There is about a 5:1 male to female predominance and for whatever reason, it is most frequent in first-born males. Usually manifests as nonbilious projectile vomiting that progresses over time. An experienced clinician will often palpate an olive shaped mass in the region of the pylorus and treatment is surgical.
Findings in this case are classic on US with thickened (> 3 mm single wall thickness) pyloric muscular wall and elongated (>15-18 mm depending on how sensitive you want to be) pyloric channel. The first image also shows a \"target sign\" appearance. There have also been calculations based upon pyloric volume, but these are relatively impractical. Most important is to do real-time imaging and identify minimal flow of fluid through the pylorus. Remember to have the patient drinking formula at the time of the examination.
UGI findings include similar findings and there are a plethora of findings described for this condition including: Mushroom sign (appearance of duodenal bulb), teat sign (pointing of the antrum), caterpillar sign (multiple hyper-active muscular contractions in the stomach), shoulder sign (shouldering of the antrum), and diamond sign (focal pointed outpouching in the pyloric channel, which often has a double or triple track appearance). Bottom line is that it is usually obvious if it is there and if you are struggling, it is probably negative. There is actually an adult form as well, although this is less common.
Ultrasound Images