Despite being preventable, colorectal cancer (CRC) is one of the leading causes of cancer deaths in the United States. Colonoscopy has been the predominant option for screening and identifying precancerous polyps, but multitarget stool DNA (mt-sDNA) has gained popularity in recent years due to its non-invasive nature. At UW Health, another non-invasive option, CT Colonography (CTC), is available; and according to data from a 20-year-long program led by Perry Pickhardt, MD and David Kim, MD, it may be the best option for many patients.
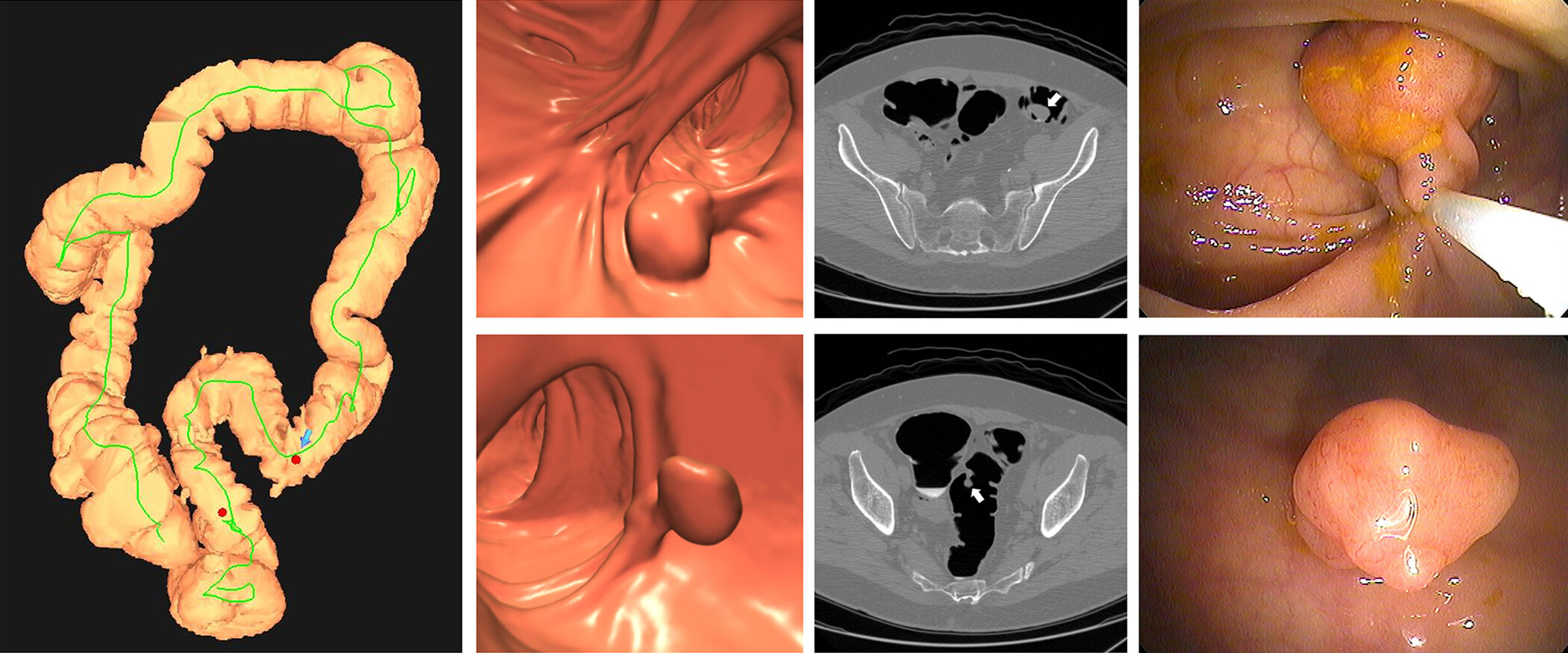
Unlike colonoscopy, there’s no risk of bleeding or perforating the colon associated with CTC. Instead of a scope, computed tomography scans are used to create 3D images of a patient’s colon from different angles. Patients are able to resume normal activities and even drive themselves home following the procedure. If polyps are detected, same-day GI Clinic services are available for polypectomies.
While stool testing is also a non-invasive screening method, CTC outperforms it in a crucial area: detecting precancerous polyps. By identifying and removing these types of polyps, patients can effectively prevent cancer that they may have developed later in life.
20 Years of Insight
The CTC screening program was established in 2004 and has completed over 15,000 CTC exams, including over 9,000 primary asymptomatic screening exams, in nearly 12,000 patients. Notably, it is the largest and longest running CTC data set in the country.
This summer, Drs. Pickhardt and Kim published “CT Colonography for Colorectal Cancer Screening and Prevention: 20-Year Programmatic Experience at a U.S. Academic Medical Center” in the American Journal of Roentgenology (AJR). Insights support CTC as a safe, noninvasive way to detect and prevent CRC. Dr. Pickhardt discussed the study with AJR Editor in Chief Andrew Rosenkrantz, MD.
Key findings from the study include:
- A polyp ≥ 6 mm was detected in 15.9% of examinations, and polyp detection had a positive predictive value of 91.6%.
- 0.2% of examinations detected histologically confirmed adenocarcinoma, yet 4% detected histologically confirmed advanced adenoma, which is considered a CRC precursor
- Additionally, CTC detected in this group unsuspected extracolonic malignancies in 0.4% of examinations and abdominal aortic aneurysm in 0.3% of examinations.
- No major complications occurred after any examination
Clinical Implementation
The department has seen success with the CTC screening program; however, the study shows that there’s been a decrease in the number of scans performed in recent years. Despite widespread insurance coverage, including Medicare coverage, CTC has been slow to gain traction as a screening option nationwide.
In the AJR Conversations podcast episode “CT Colonography for Colorectal Cancer Screening” Dr. Kim discussed some of the barriers for clinical implementation of CTC with AJR Gastrointestinal Imaging Section Editor Federica Vernuccio, MD, PhD. He noted that acceptance from primary care providers, hesitancy among radiologists, and the need for quality training as key factors to overcome.
Dr. Kim acknowledged that while hesitancy to incorporate a new exam into a practice is understandable, there is a robust body of literature supporting CTC as a safe and effective screening method that excels at detecting and preventing CRC. He highlighted that now that coverage is widespread, it’s up to radiologists to advocate for CTC screening.
“We need radiologists to champion CTC use. If radiologists don’t accept it in general throughout the world, then it will never get into widespread use. You need to get down into the local level, talk to your primary care physicians, and explain the test; what it can do and engage your primary care physicians. Otherwise, that referral will never happen.”
In the same conversation, Dr. Kim emphasized that regardless of method, screening levels for CRC remain low. An acceptable screening level is considered to be about 80% adherence rate for a given population, and many institutions are within a range of high 60s to low 70s. Widespread implementation of CTC could help close this screening gap and reduce the overall rate of CRC occurrence.
Opportunistic Screening
Comparisons can be drawn and advantages weighed between the various CRC screening methods, but opportunistic screening is a benefit gained from CTC which neither colonoscopy nor stool screening can offer. It’s the practice of reviewing medical images taken for one concern and evaluating them to potentially identify other health conditions.
CT scans taken for CRC screening can show characteristics like bone mineral density, skeletal muscle, liver fat, and aortic plaque; which can be used to evaluate the patient’s overall health and wellness. In his interview with AJR discussing the 20-year CTC program, Dr. Pickhardt acknowledged that opportunistic screening does take additional time. However, he noted that artificial intelligence (AI) tools can aid radiologists in reading opportunistic screening studies.
“I think the opportunistic CT screening revolution is just getting started. Screening for things like colorectal cancer and lung cancer fit in perfectly with this approach. I think as all radiologists are by now aware, body CT scans contain very rich cardiometabolic health information and that using these explainable AI algorithms, we can now efficiently and objectively assess these.”